Many of the top-selling drugs in America are direct beneficiaries of their manufacturers’ success in extending monopolies, with layers of patents and multi-year litigation that keeps approved generics and biosimilars off the market. Often, the larger the drug’s revenues, the safer the franchise because the potential damages could be devastating to would-be competitors if they launch “at risk” and the courts uphold the originator’s claims. As a result, the two parties may reach anti-competitive settlements because it is more lucrative for generic competitors to be paid to delay entry than try to compete or to lose the case and wait even longer.
Issue Area
Abuses of Government Programs and Regulations

Industry exploitation of policy loopholes has resulted in higher prices for patients and outsize profits for manufacturers and other stakeholders
Policies intended to protect drug innovation and provide treatment access for America's most vulnerable populations have been exploited by the biopharmaceutical industry and other supply chain stakeholders for decades, which has resulted in excessive profits and contributed to the rapid rise in drug costs for patients.
The FDA grants a period of market exclusivity, which extends 5 years of monopoly pricing for new chemical entities (NCE) and 12 years for biologic drugs in exchange for developing the new drug. Innovator companies, however, have been known to delay or impede generic and biosimilar competition through legal tactics: create patent hedges for tweaks to formulations or arguably minor additions to the overall drug, protract litigation, and engage in settlements with generic companies to delay their entry. Because a manufacturer has nearly full discretion over the price at which the drug is launched into the market, mitigating competition allows them to price high and even increase its price as the prospect of generic competition nears.
Other government policies, such as the 340B Program and Orphan Drug Act, have been exploited by health care companies in various ways. Health care providers with a 340B designation for low-income and uninsured patients purchase drugs at a discount mandated by the terms of the program and can charge for its list price plus markup. Because the designation is transferable within a health system, hospitals serving higher income patients can acquire 340B hospitals and purchase drugs at that discount, anywhere from 13% to 23.1%. The loophole within this program continues to generate billions of dollars in profit.
The Orphan Drug Act was created to incentivize manufacturers to develop drugs that treat rare diseases, or diseases affecting less than 200,000 people. Drugs with an "orphan" designation receive millions in federal taxpayer subsidies and a 7-year extension on its market exclusivity, and often get a fast track designation that expedites its review process. Manufacturers have increasingly taken existing drugs and applied for the orphan designation through a disease subtype, a process described as "salami slicing". By staggering supplemental drug applications and stacking exclusivity periods, manufacturers are able to hold off competition and command premium specialty pricing over a protracted period of time.
"Evergreening" strategies for blockbuster drugs are key sources of revenue
Layers of patents and multi-year litigation keep FDA-approved generics and biosimilars off the market
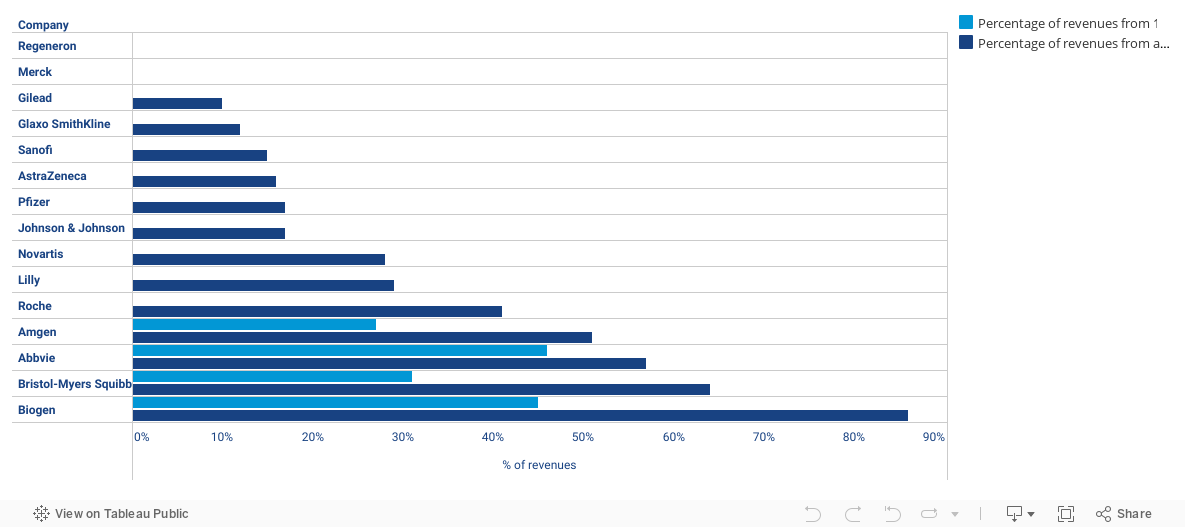
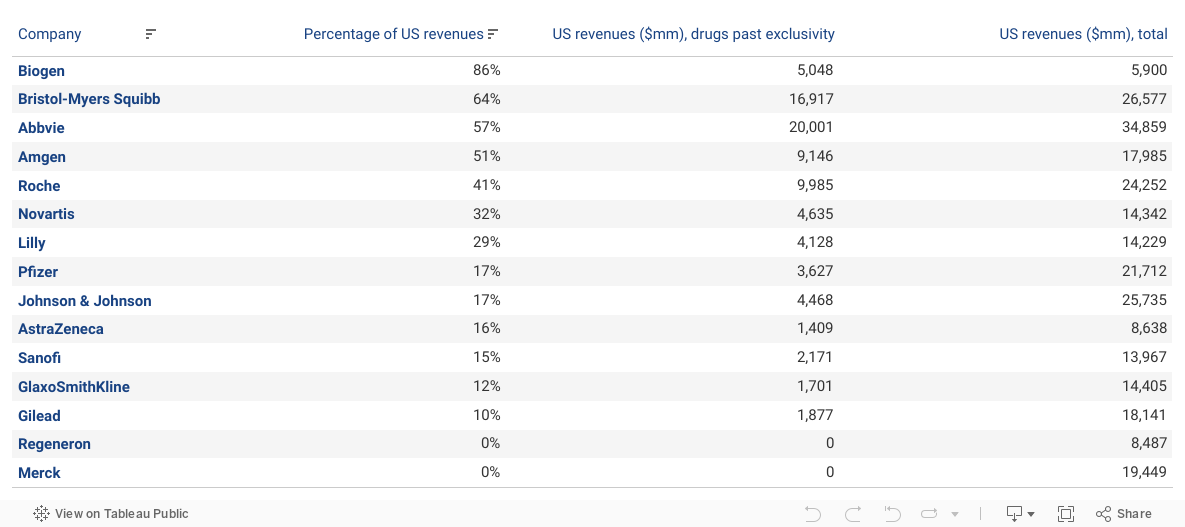
Of the 15 largest global pharmaceutical companies, four generated over 50% of their US revenues from products with expired exclusivity. For each of these, a single (very well-protected) product stands out.
- Biogen’s Tecfidera, $2.7 billion, 45% of US revenues
- Abbvie’s Humira, $16 billion, 46% of US revenues
- Amgen’s Enbrel, $4.9 billion, 27% of US revenues
- Bristol Myer’s (formerly Celgene’s) Revlimid, $8.3 billion, 31% of US revenues
Graph 1
Contribution to 2020 Sales by Drugs Past Exclusivity
Expansion of 340B Program Pads Profits for Hospitals Without Benefiting Many Patients
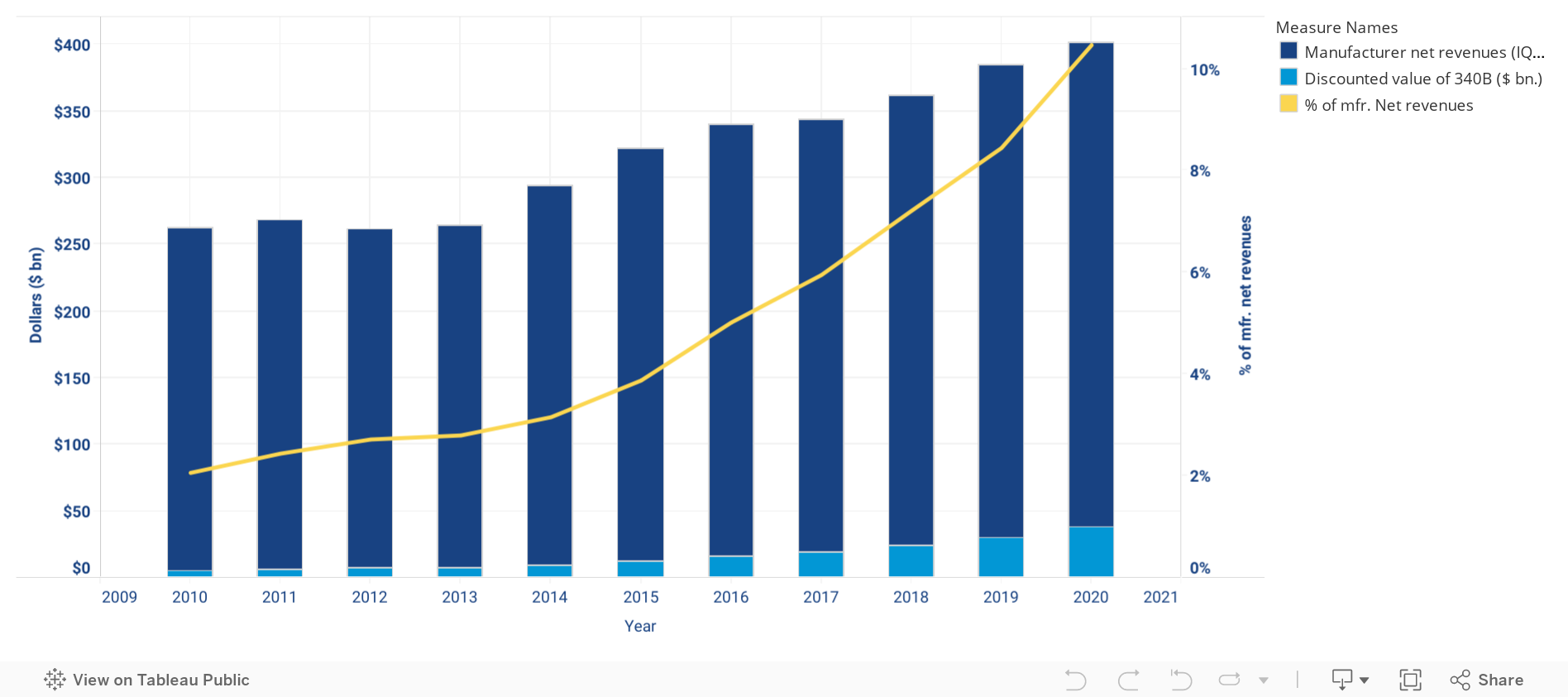
Section 340B of the Public Health Service Act was conceived 30 years ago as a policy that allowed certain hospitals that cared for low-income or uninsured patients to obtain drugs for their patients at 13% to 23.1% off the list price, or capped at Medicaid Best Price.1 While the program requires manufacturers participating in Medicaid to sell outpatient drugs at discounts, drug purchases under the 340B program in recent years have been growing in excess of 25% per year and now account for over 10% of the drug market according to some estimates. In an Adam Fein report, the program has grown to ~$38 billion and is now larger than the entire Medicaid outpatient drug market.2
While noble in concept, much of the growth of the program is a result of consolidation and the creation of extensive networks among hospitals, providers, and pharmacies, which has enabled many providers and pharmacies outside of the intended scope to procure drugs at the mandated 340B discount. As there is no requirement to pass the lower price on to patients (many of whom are insured), the contract pharmacies and hospitals often profit from the spread between their procurement cost and the reimbursement they receive.
Since the 340B program drives down the acquisition costs of drugs but not their reimbursement, it can influence the costs of patient care in several ways. It is generally acknowledged that profits resulting from the spread between a product’s acquisition cost and its reimbursement price can incentivize physicians to prescribe those products with higher profit margins (as a result of buy-and-bill purchasing). Moreover, when the cancer drug or medication is administered in hospital-based infusion suites, the overall cost to both the insurer and the patient can be significantly higher since the coinsurance is usually a percentage of the list price. The 340B discounts are effectively a diversion of funds from the manufacturers to the hospitals, clinics, and contract pharmacies that dispense and administer the drugs. In 2020, discounts provided through the program made up approximately 20% of total manufacturer rebates and discounts.2 As a result, the manufacturers have an incentive to offset these revenue losses by raising list prices so that the net revenues can be preserved.
Graph 1
Purchases under 340B Program

References
1.
RAND Corporation. The 340B Prescription Drug Discount Program. 2014. https://www.rand.org/pubs/perspectives/PE121.html
2.
Fein AJ. EXCLUSIVE: The 340B Program Soared to $38 Billion in 2020—Up 27% vs. 2019. Drug Channels. June 2021. https://www.drugchannels.net/2021/06/exclusive-340b-program-soared-to-38.html.


